If you cannot view this email,please click here
 Baby Friendly Hospital Initiative Hong Kong Association Baby Friendly Hospital Initiative Hong Kong Association |
|
|
|
|
|
Recurrent Blockage of Milk Ducts: Can it be prevented? Does compression help?
Ms Wong Nga Wai Agnes
RN, IBCLC, Trainer (WHO BF Course)

Mrs. Chan, a working mother of a 10- month-old boy, suffered from her second major episode of blocked milk ducts 2 months after the first attack. She was frustrated and wanted to stop breastfeeding.
This article illustrates the importance of taking a detailed breastfeeding and pumping history in order to identify the underlying causes of recurrent blockage of milk ducts and recommend effective preventive measures. Strategies in resolving blocked ducts are discussed.
Case History
Mrs. Chan, a working mother of a 10-month-old-baby boy, suffered from her second major episode of blocked milk ducts on the first day of returning to work after the Easter Holidays. As she had a traumatic experience of having had a breast massage to relieve the blockage in the last episode, she was worried about having to go through the same experience again and wondered whether to stop breastfeeding (BF) altogether to avoid future attacks.
Mrs. Chan described her experience of BF as uneventful and pain free all along, except for these episodes. Her usual BF / pumping schedule was reported as follows: Direct BF before leaving for work; pumping twice, yielding 150 – 180ml per session at her workplace during the day; and direct BF twice (with both breasts per feed) in the evening. The last feed was between 10 and 11 pm, after which the baby slept through the night. During the Easter holidays, Mrs. Chan had been directly breastfeeding her baby on demand, with one or both breasts per feed, for about 6 – 7 times a day. She thought some of these feeds could have been comfort feeds as the baby had been taking solid feeds satisfactorily.
A very similar episode involving her right breast occurred on the first day of returning to work after the Lunar New Year holidays, about 2 months before. The BF / pumping history was basically the same as currently. At the time, she consulted a “lactation specialist”, who conducted two sessions of breast massage, after which the blockage resolved. She recalled the breast massage was very painful and bruises appeared afterwards.
Another minor episode of blocked ducts occurred when her baby first started to sleep through the night at around 4 – 5 months of age. Mrs. Chan was then pumping breastmilk twice during the day at the workplace. Luckily, the blocked ducts resolved quickly as she encouraged her baby to suckle more frequently on the affected side and she woke up to pump for a few nights to relieve the full breasts.
On physical examination, the mother wore loose clothing and a wireless bra. There was a slightly tender breast lump measuring 2cm at the 11 o’clock position of her left breast. The overlying skin was normal.
What are the causes of Mrs. Chan’s blocked milk ducts?
Without timely and effective removal of milk, blockage of milk ducts can occur. Ineffective milk removal can be due to improper latching or the use of an ineffective pump. Milk can also be trapped in a compressed or damaged duct due to pressure from an unfit nursing bra especially with underwire, or from sleeping on the stomach. Factors contributing to a sudden decrease in feeding or pumping frequency such as normal changes in the baby’s sleep-feeding pattern; maternal or baby illnesses; and mother’s busy activity or work schedule; etc. are also important. In particular, the mother’s busy scheduling does not only mean untimely removal of milk, but the related maternal stress also lowers the production of oxytocin, the hormone that causes the breasts to eject milk. Omitting or delaying feeding or pumping is the commonest cause of recurrent blockage of milk ducts observed in the Maternal and Child Health Centres.
Baby sleeping through the night without feeding
It is not uncommon for a breastfeeding mother, especially with copious milk supply, to have minor blocked ducts when her few-months-old baby begins to sleep through the night. Excessive milk, not removed from the breast, triggers the autocrine feedback mechanism to down-regulate the milk supply. In the meantime, milk stasis increases the likelihood of blockage of ducts, which often presents as mildly painful small lump(s). These usually resolve within a few days if milk removal is effective. One or two days of simple analgesic are often helpful. However, further assessments would be needed when the blocked ducts do not improve within 2 days.
In this case, Mrs. Chan had appropriately continued demand feeding during the day while encouraging suckling on the affected side. In the first couple of nights, she had woken up to relieve the breast fullness by pumping. These had helped to gradually adjust her milk supply to fit the baby’s new feeding schedule while resolving the blockage through effective milk removal by the baby.
Sudden changes in feeding schedule
For Mrs. Chan, both major episodes of blocked ducts had occurred on the first working day after the long holidays. It was notable that she had switched to more frequent direct BF during the long holidays and returned to the usual schedule upon returning to work. It is conceivable that more frequent suckling during the long holidays had stimulated an increase in milk supply. When she returned to work, a less frequent schedule of milk removal had resulted in fullness of her breasts and milk stasis. Besides, work stress might have further impeded the production of oxytocin. Both had contributed to the occurrence of blocked ducts. Therefore, to prevent future attacks, on the first few days of returning to work from long holidays, Mrs. Chan should pump or express breastmilk more frequently during the day to prevent her breasts from being too full.
What is the most effective way to relieve blocked milk ducts?
Many mothers with blocked ducts have tried resolving the problem by breast massage: in form of compressing +/- squeezing the breast / lumps either by themselves or with the help of “lactation specialists”. As the milk ducts are located beneath the skin, compression with considerable force is needed to push the milk plugs through. Although this may help in some mothers, such manipulation can potentially traumatize the breast tissues, in addition to causing intense pain.
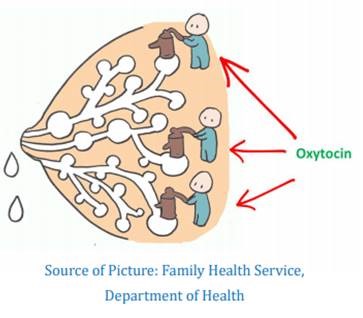
There are pain-free and more effective strategies in resolving the blocked ducts. Let us revisit the physiology of milk ejection (let-down) reflex: When the nipple is stimulated by the baby’s suckling or pumping, oxytocin is released in a pulsatile manner into the blood stream from the posterior pituitary gland. Oxytocin causes the myoepithelial cells around the alveoli to contract and squeeze the milk down the ducts. It also shortens and widens the milk ducts, facilitating the milk to flow down easily. Therefore, amplifying the milk ejection reflex, analogous to a natural “internal pump”, is the physiological and effective way in resolving blocked ducts. Apart from tactile stimulation of the nipple, seeing, hearing or simply thinking about the baby can also induce oxytocin secretion, while anxiety, stress, tiredness or pain would diminish its release.
To maximize this physiological pump, we may advise the mother to:
Reduce the pain: Adequate pain relief is important because pain inhibits the milk ejection reflex. The mother may take simple analgesics +/- cold compress.
Relax: The mother should breastfeed or express her breastmilk in a comfortable position and relaxing environment. Listening to music, breathing slowly and deeply, keeping warm and/or drinking something warm are often helpful. Some mothers may prefer a warm shower or placing a warm face-steamer on her breast before breastfeeding.
Gently perform breast massage and nipple stimulation: Before milk removal, gentle breast massage and rolling the nipple between fingers can stimulate the milk ejection reflex. During milk removal, the affected breast can be massaged gently by stroking from behind the lump towards the nipple with the palm or shaft of fingers to further improve the milk flow.
Think about the baby: During breastfeeding or pumping, the mother may keep her baby close to her through skin-to-skin contact. When pumping in the workplace, thinking about her baby or looking at her baby’s photo can be very helpful.
Get the support of her spouse: Last but not least, inviting the husband (or other suitable persons) to perform gentle back massage can be very useful in soothing and relaxing a stressful and tiring mother.
In sum, GENTLE massage with amplified milk ejection reflex is a powerful tool to resolve blocked ducts. Breast massage with forceful compression should be avoided.
Key Message:
Key points in the management of blocked milk duct:
- Reduce pain by analgesics +/- cold compress
- Amplify the milk ejection reflex (avoid forceful breast massage)
- Ensure frequent and effective milk removal
- Relieve stress and ensure adequate rest
- Avoid tight clothing
- Monitor closely by professionals
處理乳管阻塞的要點:
- 使用止痛藥物+/-凍敷減痛
- 加強噴奶反射 (避免大力擠壓乳房)
- 確保頻密及有效地排(擠)出乳汁
- 減輕壓力,保持輕鬆,確保休息足夠
- 避免穿著過緊衣服
- 讓專業人士密切監察情況
|
Views expressed in this article are the author's and do not necessarily reflect the opinion or position of the BFHIHKA.
作者在本文章表達的見解,未必代表愛嬰醫院香港協會的意見或立場
Editor-in-Chief: Dr Shirley Leung
Editorial Team: Dr Amy WH Fung, Ms Iris SL Ip, Ms Helen YN Leung, Ms Agnes NW Wong, Dr Sandra YW Yau, Ms Amy KM Yeung
Illustration: Ms Cheryl Young
Please click here to download the whole article and visit our website to subscribe our E-newsletter

|
|
|
|
|
|
|
|
Baby Friendly Hotline: 2838 7727 (9am-9pm)
General Enquiry: 2591 0782
Address: 7th Floor, SUP Tower, 75-83 King’s Road, Hong Kong
|
|
|
|
愛嬰醫院香港協會,版權所有。
All rights reserved by Baby Friendly Hospital Initiative Hong Kong Association.
|
|
|
|
|